Google’s artificial intelligence company DeepMind has published „really significant“ research showing its algorithm can identify around 50 eye diseases by looking at retinal eye scans.
DeepMind said its AI was as good as expert clinicians, and that it could help prevent people from losing their sight.
DeepMind has been criticised for its practices around medical data, but cofounder Mustafa Suleyman said all the information in this research project was anonymised.
The company plans to hand the technology over for free to NHS hospitals for five years, provided it passes the next phase of research.
Google’s artificial intelligence company, DeepMind, has developed an AI which can successfully detect more than 50 types of eye disease just by looking at 3D retinal scans.
DeepMind published on Monday the results of joint research with Moorfields Eye Hospital, a renowned centre for treating eye conditions in London, in Nature Medicine.
The company said its AI was as accurate as expert clinicians when it came to detecting diseases, such as diabetic eye disease and macular degeneration. It could also recommend the best course of action for patients and suggest which needed urgent care.
A technician examines an OCT scan.DeepMind
What is especially significant about the research, according to DeepMind cofounder Mustafa Suleyman, is that the AI has a level of „explainability“ that could boost doctors‘ trust in its recommendations.
„It’s possible for the clinician to interpret what the algorithm is thinking,“ he told Business Insider. „[They can] look at the underlying segmentation.“
In other words, the AI looks less like a mysterious black box that’s spitting out results. It labels pixels on the eye scan that corresponds to signs of a particular disease, Suleyman explained, and can calculate its confidence in its own findings with a percentage score. „That’s really significant,“ he said.
DeepMind’s AI analysing an OCT scan.DeepMind
Suleyman described the findings as a „research breakthrough“ and said the next step was to prove the AI works in a clinical setting. That, he said, would take a number of years. Once DeepMind is in a position to deploy its AI across NHS hospitals in the UK, it will provide the service for free for five years.
Patients are at risk of losing their sight because doctors can’t look at their eye scans in time
British eye specialists have been warning for years that patients are at risk of losing their sight because the NHS is overstretched, and because the UK has an ageing population.
Part of the reason DeepMind and Moorfields took up the research project was because clinicians are „overwhelmed“ by the demand for eye scans, Suleyman said.
„If you have a sight-threatening disease, you want treatment as soon as possible,“ he explained. „And unlike in A&E, where a staff nurse will talk to you and make an evaluation of how serious your condition is, then use that evaluation to decide how quickly you are seen. When an [eye] scan is submitted, there isn’t a triage of your scan according to its severity.“
A patient having an OCT scan.DeepMind
Putting eye scans through the AI could speed the entire process up.
„In the future, I could envisage a person going into their local high street optician, and have an OCT scan done and this algorithm would identify those patients with sight-threatening disease at the very early stage of the condition,“ said Dr Pearse Keane, consultant ophthalmologist at Moorfields Eye Hospital.
DeepMind’s AI was trained on a database of almost 15,000 eye scans, stripped of any identifying information. DeepMind worked with clinicians to label areas of disease, then ran those labelled images through its system. Suleyman said the two-and-a-half project required „huge investment“ from DeepMind and involved 25 staffers, as well as the researchers from Moorfields.
People are still worried about a Google-linked company having access to medical data
While DeepMind has remained UK-based and independent from Google, the relationship has attracted scrutiny. The main question is whether Google, a private US company, should have access to the sensitive medical data required for DeepMind’s health arm.
„You can’t identify whose scans it was. We’re in quite a different regime, this is very much research, and we’re a number of years from being able to deploy in practice,“ he said.
Suleyman added: „How this has the potential to have transform the NHS is very clear. We’ve been very conscious that this will be a model that’s published, and available to others to implement.
„The labelled dataset is available to other researchers. So this is very much an open and collaborative relationship between equals that we’ve worked hard to foster. I’m proud of that work.“
Researchers at MIT, the University of Sheffield, and the Tokyo Institute of Technology have demonstrated a tiny origami robot that can unfold itself from a swallowed capsule and, steered by external magnetic fields, crawl across the stomach wall to remove a swallowed button battery or patch a wound.
Click to Open Overlay GalleryBuried deep within each cell in Sergey Brin’s body—in a gene called LRRK2, which sits on the 12th chromosome—is a genetic mutation that has been associated with higher rates of Parkinson’s. Rafa JennSeveral evenings a week, after a day’s work at Google headquarters in Mountain View, California, Sergey Brin drives up the road to a local pool. There, he changes into swim trunks, steps out on a 3-meter springboard, looks at the water below, and dives.
Brin is competent at all four types of springboard diving—forward, back, reverse, and inward. Recently, he’s been working on his twists, which have been something of a struggle. But overall, he’s not bad; in 2006 he competed in the master’s division world championships. (He’s quick to point out he placed sixth out of six in his event.)
The diving is the sort of challenge that Brin, who has also dabbled in yoga, gymnastics, and acrobatics, is drawn to: equal parts physical and mental exertion. “The dive itself is brief but intense,” he says. “You push off really hard and then have to twist right away. It does get your heart rate going.”
There’s another benefit as well: With every dive, Brin gains a little bit of leverage—leverage against a risk, looming somewhere out there, that someday he may develop the neurodegenerative disorder Parkinson’s disease. Buried deep within each cell in Brin’s body—in a gene called LRRK2, which sits on the 12th chromosome—is a genetic mutation that has been associated with higher rates of Parkinson’s.
Not everyone with Parkinson’s has an LRRK2 mutation; nor will everyone with the mutation get the disease. But it does increase the chance that Parkinson’s will emerge sometime in the carrier’s life to between 30 and 75 percent. (By comparison, the risk for an average American is about 1 percent.) Brin himself splits the difference and figures his DNA gives him about 50-50 odds.
That’s where exercise comes in. Parkinson’s is a poorly understood disease, but research has associated a handful of behaviors with lower rates of disease, starting with exercise. One study found that young men who work out have a 60 percent lower risk. Coffee, likewise, has been linked to a reduced risk. For a time, Brin drank a cup or two a day, but he can’t stand the taste of the stuff, so he switched to green tea. (“Most researchers think it’s the caffeine, though they don’t know for sure,” he says.) Cigarette smokers also seem to have a lower chance of developing Parkinson’s, but Brin has not opted to take up the habit. With every pool workout and every cup of tea, he hopes to diminish his odds, to adjust his algorithm by counteracting his DNA with environmental factors.
“This is all off the cuff,” he says, “but let’s say that based on diet, exercise, and so forth, I can get my risk down by half, to about 25 percent.” The steady progress of neuroscience, Brin figures, will cut his risk by around another half—bringing his overall chance of getting Parkinson’s to about 13 percent. It’s all guesswork, mind you, but the way he delivers the numbers and explains his rationale, he is utterly convincing.
Brin, of course, is no ordinary 36-year-old. As half of the duo that founded Google, he’s worth about $15 billion. That bounty provides additional leverage: Since learning that he carries a LRRK2 mutation, Brin has contributed some $50 million to Parkinson’s research, enough, he figures, to “really move the needle.” In light of the uptick in research into drug treatments and possible cures, Brin adjusts his overall risk again, down to “somewhere under 10 percent.” That’s still 10 times the average, but it goes a long way to counterbalancing his genetic predisposition.
It sounds so pragmatic, so obvious, that you can almost miss a striking fact: Many philanthropists have funded research into diseases they themselves have been diagnosed with. But Brin is likely the first who, based on a genetic test, began funding scientific research in the hope of escaping a disease in the first place.
His approach is notable for another reason. This isn’t just another variation on venture philanthropy—the voguish application of business school practices to scientific research. Brin is after a different kind of science altogether. Most Parkinson’s research, like much of medical research, relies on the classic scientific method: hypothesis, analysis, peer review, publication. Brin proposes a different approach, one driven by computational muscle and staggeringly large data sets. It’s a method that draws on his algorithmic sensibility—and Google’s storied faith in computing power—with the aim of accelerating the pace and increasing the potential of scientific research. “Generally the pace of medical research is glacial compared to what I’m used to in the Internet,” Brin says. “We could be looking lots of places and collecting lots of information. And if we see a pattern, that could lead somewhere.”
In other words, Brin is proposing to bypass centuries of scientific epistemology in favor of a more Googley kind of science. He wants to collect data first, then hypothesize, and then find the patterns that lead to answers. And he has the money and the algorithms to do it.
Click to Open Overlay GalleryGiven what seems like very bad news, most of us would actually do what Brin did: Go over our options, get some advice, and move on with life. Nathan Fox
Brin’s faith in the power of numbers—and the power of knowledge, more generally—is likely something he inherited from his parents, both scientists. His father, Michael, is a second-generation mathematician; his mother Eugenia is trained in applied mathematics and spent years doing meteorology research at NASA. The family emigrated from Russia when Brin was 6. At 17, he took up mathematics himself at the University of Maryland, later adding a second major in computer science. When he reached Stanford for his PhD—a degree he still hasn’t earned, much to his parents’ chagrin—he focused on data mining. That’s when he began thinking about the power of large data sets and what might come of analyzing them for unexpected patterns and insights.
Around the same time, in 1996, Brin’s mother started to feel some numbness in her hands. The initial diagnosis was repetitive stress injury, brought on by years of working at a computer. When tests couldn’t confirm that diagnosis, her doctors were stumped. Soon, though, Eugenia’s left leg started to drag. “It was just the same as my aunt, who had Parkinson’s years ago,” she recalls. “The symptoms started in the same way, at the same age. To me, at least, it was obvious there was a connection.”
At the time, scientific opinion held that Parkinson’s was not hereditary, so Brin didn’t understand his mother’s concern. “I thought it was crazy and completely irrational,” he says. After further tests at Johns Hopkins and the Mayo Clinic, though, she was diagnosed with Parkinson’s in 1999.
Even after the LRRK2 connection was made in 2004, Brin still didn’t connect his mother’s Parkinson’s to his own health. Then, in 2006, his wife-to-be, Anne Wojcicki, started the personal genetics company 23andMe (Google is an investor). As an alpha tester, Brin had the chance to get an early look at his genome. He didn’t find much of concern. But then Wojcicki suggested he look up a spot known as G2019S—the notch on the LRRK2 gene where an adenine nucleotide, the A in the ACTG code of DNA, sometimes substitutes for a guanine nucleotide, the G. And there it was: He had the mutation. His mother’s 23andMe readout showed that she had it, too.
Brin didn’t panic; for one thing, his mother’s experience with the disease has been reassuring. “She still goes skiing,” he says. “She’s not in a wheelchair.” Instead, he spent several months mulling over the results. He began to consult experts, starting with scientists at the Michael J. Fox Foundation and at the Parkinson’s Institute, which is not far from Google’s headquarters. He quickly realized it was going to be impractical to keep his risk from the public. “I can’t talk to 1,000 people in secret,” he says. “So I might as well put it out there to the world. It seemed like information that was worthy of sharing and might even be interesting.”
So one day in September 2008, Brin started a blog. His first post was called simply “LRRK2.”
“I know early in my life something I am substantially predisposed to,” Brin wrote. “I now have the opportunity to adjust my life to reduce those odds (e.g., there is evidence that exercise may be protective against Parkinson’s). I also have the opportunity to perform and support research into this disease long before it may affect me. And, regardless of my own health, it can help my family members as well as others.”
Brin continued: “I feel fortunate to be in this position. Until the fountain of youth is discovered, all of us will have some conditions in our old age, only we don’t know what they will be. I have a better guess than almost anyone else for what ills may be mine—and I have decades to prepare for it.”
In a sense, we’ve been using genetics to foretell disease risk forever. When we talk about “family history,” we’re largely talking about DNA, about how our parents’ health might hint at our own. A genetic scan is just a more modern way to link our familial past with our potential future. But there’s something about the precision of a DNA test that can make people believe that chemistry is destiny—that it holds dark, implacable secrets. This is why genetic information is sometimes described as “toxic knowledge”: Giving people direct access to their genetic information, in the words of Stanford bioethicist Hank Greely, is out and out “reckless.”
It’s true that in the early days of the science, genetic testing meant learning about a dreaded degenerative disease like Huntington’s or cystic fibrosis. But these diseases, although easy to identify, are extremely rare. Newer research has shown that when it comes to getting sick, a genetic predisposition is usually just one factor. The vast majority of conditions are also influenced by environment and day-to-day habits, areas where we can actually take some action.
But, surprisingly, the concept of genetic information as toxic has persisted, possibly because it presumes that people aren’t equipped to learn about themselves. But research shows this presumption to be unfounded. In 2009, The New England Journal of Medicine published results of the Risk Evaluation and Education for Alzheimer’s Disease study, an 11-year project that sought to examine how people react to finding out that they have a genetic risk for Alzheimer’s. Like Parkinson’s, Alzheimer’s is a neurodegenerative condition centering on the brain. But unlike Parkinson’s, Alzheimer’s has no known treatment. So learning you have a genetic predisposition should be especially toxic.
In the study, a team of researchers led by Robert Green, a neurologist and geneticist at Boston University, contacted adults who had a parent with Alzheimer’s and asked them to be tested for a variation in a gene known as ApoE. Depending on the variation, an ApoE mutation can increase a person’s risk for Alzheimer’s from three to 15 times the average. One hundred sixty-two adults agreed; 53 were told they had the mutation.
The results were delivered to the participants with great care: A genetic counselor walked each individual through the data, and all the subjects had follow-up appointments with the counselor. Therapists were also on call. “People were predicting catastrophic reactions,” Green recalls. “Depression, suicide, quitting their jobs, abandoning their families. They were anticipating the worst.”
But that isn’t what happened. People told that they were at dramatically higher risk for developing Alzheimer’s later in life seemed to process the information and integrate it into their lives, often choosing to lead more healthy lifestyles. “People are handling it,” Green says. “It doesn’t seem to be producing any clinically apparent distress.”
In other experiments, Green has further challenged the conventional wisdom about the toxicity of genetic information: He has begun questioning the need for counselors and therapists. “We’re looking at what happens if you don’t do this elaborate thing. What if you do it like a lab test in your doctor’s office? We’re treating it more like cholesterol and less like Huntington’s disease.”
In other words, given what seems like very bad news, most of us would do what Sergey Brin did: Go over our options, get some advice, and move on with life. “Everyone’s got their challenges; everyone’s got something to deal with,” Brin says. “This is mine. To me, it’s just one of any number of things that I could get in old age. And the most important factor is that I can do something about it.”
High-Speed Science
Can a model fueled by data sets and computational power compete with the gold standard of research? Maybe: Here are two timelines—one from an esteemed traditional research project run by the NIH, the other from the 23andMe Parkinson’s Genetics Initiative. They reached almost the same conclusion about a possible association between Gaucher’s disease and Parkinson’s disease, but the 23andMe project took a fraction of the time.—Rachel Swaby
Traditional Model
1. Hypothesis: An early study suggests that patients with Gaucher’s disease (caused by a mutation to the GBA gene) might be at increased risk of Parkinson’s.
2. Studies: Researchers conduct further studies, with varying statistical significance.
3. Data aggregation: Sixteen centers pool information on more than 5,500 Parkinson’s patients.
4. Analysis: A statistician crunches the numbers.
5. Writing: A paper is drafted and approved by 64 authors.
6. Submission: The paper is submitted to The New England Journal of Medicine. Peer review ensues.
7. Acceptance:NEJM accepts the paper.
8. Publication: The paper notes that people with Parkinson’s are 5.4 times more likely to carry the GBA mutation.
Total time elapsed: 6 years
Parkinson’s Genetics initiative
1. Tool Construction: Survey designers build the questionnaire that patients will use to report symptoms.
2. Recruitment: The community is announced, with a goal of recruiting 10,000 subjects with Parkinson’s.
3. Data aggregation: Community members get their DNA analyzed. They also fill out surveys.
4. Analysis: Reacting to the NEJM paper, 23andMe researchers run a database query based on 3,200 subjects. The results are returned in 20 minutes.
5. Presentation: The results are reported at a Royal Society of Medicine meeting in London: People with GBA are 5 times more likely to have Parkinson’s, which is squarely in line with the NEJM paper. The finding will possibly be published at a later date.
Total time elapsed: 8 months
If Brin’s blog post betrayed little fear about his risk for Parkinson’s, it did show a hint of disappointment with the state of knowledge on the disease. (His critique was characteristically precise: “Studies tend to have small samples with various selection biases.”)
His frustration is well founded. For decades, Parkinson’s research has been a poor cousin to the study of Alzheimer’s, which affects 10 times as many Americans and is therefore much more in the public eye. What is known about Parkinson’s has tended to emerge from observing patients in clinical practice, rather than from any sustained research. Nearly all cases are classified as idiopathic, meaning there’s no known cause. Technically, the disease is a result of the loss of brain cells that produce the neurotransmitter dopamine, but what causes those cells to die is unclear. The classic symptoms of the condition—tremors, rigidity, balance problems—come on gradually and typically don’t develop until dopamine production has declined by around 80 percent, meaning that a person can have the disease for years before experiencing the first symptom.
As far as treatments go, the drug levodopa, which converts to dopamine in the brain, remains the most effective. But the drug, developed in 1967, has significant side effects, including involuntary movements and confusion. Other interventions, like deep-brain stimulation, are invasive and expensive. Stem cell treatments, which generated great attention and promise a decade ago, “didn’t really work,” says William Langston, director of the Parkinson’s Institute. “Transferring nerve cells into the brain and repairing the brain has been harder than anybody thought.”
There are, however, some areas of promise—including the 2004 discovery of the LRRK2 connection. It’s especially common among people of Ashkenazi descent, like Brin, and appears in just about 1 percent of Parkinson’s patients. Rare as the mutation is, however, LRRK2 cases of Parkinson’s appear indistinguishable from other cases, making LRRK2 a potential window onto the disease in general.
LRRK2 stands for leucine-rich repeat kinase. Kinases are enzymes that activate proteins in cells, making them critical to cell growth and death. In cancer, aberrant kinases are known to contribute to tumor growth. That makes them a promising target for research. Drug companies have already developed kinase inhibitors for cancer; it’s a huge opportunity for Parkinson’s treatment, as well: If overactive kinases interfere with dopamine-producing cells in all Parkinson’s cases, then a kinase inhibitor may be able to help not just the LRRK2 carriers but all people with the disease.
Another promising area for research is that delay between the loss of dopamine-producing cells and the onset of symptoms. As it stands, this lag makes treatment a much more difficult problem. “By the time somebody has full-blown Parkinson’s, it’s way too late,” Langston says. “Any number of promising drugs have failed, perhaps because we’re getting in there so late.” But doctors can’t tell who should get drugs earlier, because patients are asymptomatic. If researchers could find biomarkers—telltale proteins or enzymes detected by, say, a blood or urine test—that were produced before symptoms emerged, a drug regimen could be started early enough to work.
And indeed, Brin has given money to both these areas of research, predominantly through gifts to the Parkinson’s Institute and to the Michael J. Fox Foundation, which is committed to what’s called translational research—getting therapies from researchers to the clinic as quickly as possible. Last February the Fox Foundation launched an international consortium of scientists working on LRRK2, with a mandate for collaboration, openness, and speed. “The goal is to get people to change their behavior and share information much more quickly and openly,” says Todd Sherer, head of the Fox Foundation’s research team. “We need to change the thinking.”
As Brin’s understanding of Parkinson’s grew, though, and as he talked with Wojcicki about research models, he realized that there was an even bolder experiment in the offing.
In 1899, scientists at Bayer unveiled Aspirin, a drug it offered as an effective remedy for colds, lumbago, and toothaches, among other ills. How aspirin—or acetylsalicylic acid—actually worked was a mystery. All people knew was that it did (though a discouraging side effect, gastric bleeding, emerged in some people).
It wasn’t until the 1960s and ’70s that scientists started to understand the mechanism: Aspirin inhibits the production of chemicals in the body called prostaglandins, fatty acids that can cause inflammation and pain. That insight proved essential to understanding the later discovery, in 1988, that people who took aspirin every other day had remarkably reduced rates of heart attack—cases in men dropped by 44 percent. When the drug inhibits prostaglandins, it seems, it inhibits the formation of blood clots, as well—reducing the risk of heart attack or stroke.
The second coming of aspirin is considered one of the triumphs of contemporary medical research. But to Brin, who spoke of the drug in a talk at the Parkinson’s Institute last August, the story offers a different sort of lesson—one drawn from that period after the drug was introduced but before the link to heart disease was established. During those decades, Brin notes, surely “many millions or hundreds of millions of people who took aspirin had a variety of subsequent health benefits.” But the association with aspirin was overlooked, because nobody was watching the patients. “All that data was lost,” Brin said.
In Brin’s way of thinking, each of our lives is a potential contribution to scientific insight. We all go about our days, making choices, eating things, taking medications, doing things—generating what is inelegantly called data exhaust. A century ago, of course, it would have been impossible to actually capture this information, particularly without a specific hypothesis to guide a researcher in what to look for. Not so today. With contemporary computing power, that data can be tracked and analyzed. “Any experience that we have or drug that we may take, all those things are individual pieces of information,” Brin says. “Individually, they’re worthless, they’re anecdotal. But taken together they can be very powerful.”
In computer science, the process of mining such large data sets for useful associations is known as a market-basket analysis. Conventionally, it has been used to divine patterns in retail purchases. It’s how Amazon.com can tell you that “customers who bought X also bought Y.”
But a problem emerges as the data in a basket become less uniform. This was the focus of much of Brin’s work at Stanford, where he published several papers on the subject. One, from 1997, argued that given the right algorithms, meaningful associations can be drawn from all sorts of unconventional baskets—”student enrollment in classes, word occurrence in text documents, users’ visits of Web pages, and many more.” It’s not a stretch to say that our experiences as patients might conceivably be the next item on the list.
This is especially true given the advances in computational power since 1997, when Brin and his fellow Stanford comp-sci student Larry Page were starting Google. “When Larry and I started the company,” Brin says, “we had to get some hard drives to, you know, store the entire Web. We ended up in a back alley in San Jose, dealing with some shady guy. We spent $10,000 or $20,000, all our life savings. We got these giant stacks of hard drives that we had to fit in our cars and get home. Just last week I happened to go to Fry’s and I picked up a hard drive that was 1 terabyte and cost like $100. And it was bigger than all those hard drives put together.”
This computing power can be put to work to answer questions about health. As an example, Brin cites a project developed at his company’s nonprofit research arm, Google.org. Called Google Flu Trends, the idea is elegantly simple: Monitor the search terms people enter on Google, and pull out those words and phrases that might be related to symptoms or signs of influenza, particularly swine flu.
In epidemiology, this is known as syndromic surveillance, and it usually involves checking drugstores for purchases of cold medicines, doctor’s offices for diagnoses, and so forth. But because acquiring timely data can be difficult, syndromic surveillance has always worked better in theory than in practice. By looking at search queries, though, Google researchers were able to analyze data in near real time. Indeed, Flu Trends can point to a potential flu outbreak two weeks faster than the CDC’s conventional methods, with comparable accuracy. “It’s amazing that you can get that kind of signal out of very noisy data,” Brin says. “It just goes to show that when you apply our newfound computational power to large amounts of data—and sometimes it’s not perfect data—it can be very powerful.” The same, Brin argues, would hold with patient histories. “Even if any given individual’s information is not of that great quality, the quantity can make a big difference. Patterns can emerge.”
Brin’s tolerance for “noisy data” is especially telling, since medical science tends to consider it poisonous. Biomedical researchers often limit their experiments to narrow questions that can be rigorously measured. But the emphasis on purity can mean fewer patients to study, which results in small data sets. That limits the research’s “power”—a statistical term that generally means the probability that a finding is actually true. And by design it means the data almost never turn up insights beyond what the study set out to examine.
Increasingly, though, scientists—especially those with a background in computing and information theory—are starting to wonder if that model could be inverted. Why not start with tons of data, a deluge of information, and then wade in, searching for patterns and correlations?
This is what Jim Gray, the late Microsoft researcher and computer scientist, called the fourth paradigm of science, the inevitable evolution away from hypothesis and toward patterns. Gray predicted that an “exaflood” of data would overwhelm scientists in all disciplines, unless they reconceived their notion of the scientific process and applied massive computing tools to engage with the data. “The world of science has changed,” Gray said in a 2007 speech—from now on, the data would come first.
Gray’s longtime employer, Bill Gates, recently made a small wager on the fourth paradigm when he invested $10 million in Schrödinger, a Portland, Oregon-based firm that’s using massive computation to rapidly simulate the trial and error of traditional pharmaceutical research.
And Andy Grove, former chair and CEO of Intel, has likewise called for a “cultural revolution” in science, one modeled on the tech industry’s penchant for speedy research and development. Grove, who was diagnosed with Parkinson’s in 2000 and has since made the disease his casus belli, shakes his fist at the pace of traditional science: “After 10 years in the Parkinson’s field, we may finally have three drugs in Phase I and Phase II trials next year—that’s more than ever before. But let’s get real. We’ll get the results in 2012, then they’ll argue about it for a year, then Phase III results in 2015, then argue about that for a year—if I’m around when they’re done …” He doesn’t finish his thought. “The whole field is not pragmatic enough. They’re too nice to themselves.”
Grove disagrees somewhat with Brin’s emphasis on patterns over hypothesis. “You have to be looking for something,” he says. But the two compare notes on the disease from time to time; both are enthusiastic and active investors in the Michael J. Fox Foundation. (Grove is even known to show up on the online discussion forums.)
In the world of traditional drug research, however, there’s more than a little skepticism about swapping out established biomedical approaches for technological models. Derek Lowe, a longtime medicinal chemist and author of a widely read drug industry blog, grants that big hardware and big data can be helpful. But for a disease as opaque as Parkinson’s, he argues, the challenge of drug development will always come down to basic chemistry and biology. “I don’t have a problem with data,” Lowe says. “The problem is that the data is tremendously noisy stuff. We just don’t know enough biology. If Brin’s efforts will help us understand that, I’m all for it. But I doubt they will.”
To be sure, biomedicine, and pharmaceutical research in particular, is not the same as software or computer chips. It’s a much more complicated process, and Brin acknowledges as much: “I’m not an expert in biological research. I write a bunch of computer code and it crashes, no big deal. But if you create a drug and it kills people, that’s a different story.” Brin knows that his method will require follow-up research to get through the traditional hoops of drug discovery and approvals. But, he adds, “in my profession you really make progress based on how quick your development cycle is.”
So, with the cooperation of the Parkinson’s Institute, the Fox Foundation, and 23andMe, he has proposed a new development cycle. Brin has contributed $4 million to fund an online Parkinson’s Disease Genetics Initiative at 23andMe: 10,000 people who’ve been diagnosed with the disease and are willing to pour all sorts of personal information into a database. (They’ve tapped about 4,000 so far.) Volunteers spit into a 23andMe test tube to have their DNA extracted and analyzed. That information is then matched up with surveys that extract hundreds of data points about the volunteers’ environmental exposures, their family history, disease progression, and treatment response. The questions range from the mundane (“Are you nearsighted?”)—to the perplexing (“Have you had trouble staying awake?”). It is, in short, an attempt to create the always-on data-gathering project that Brin believes could aid all medical research—and, potentially, himself. “We have no grand unified theory,” says Nicholas Eriksson, a 23andMe scientist. “We have a lot of data.”
Click to Open Overlay GalleryWhy not do science differently? Gather tons of data, then start searching for correlations. Steven Wilson
It’s hard to overstate the difference between this approach and conventional research. “Traditionally, an experiment with 10 or 20 subjects was big,” says the Parkinson’s Institute’s Langston. “Then it went up to the hundreds. Now 1,000 subjects would be a lot—so with 10,000, suddenly we’ve reached a scale never seen before. This could dramatically advance our understanding.”
Langston offers a case in point. Last October, the New England Journal of Medicinepublished the results of a massive worldwide study that explored a possible association between people with Gaucher’s disease—a genetic condition where too much fatty substances build up in the internal organs—and a risk for Parkinson’s. The study, run under the auspices of the National Institutes of Health, hewed to the highest standards and involved considerable resources and time. After years of work, it concluded that people with Parkinson’s were five times more likely to carry a Gaucher mutation.
Langston decided to see whether the 23andMe Research Initiative might be able to shed some insight on the correlation, so he rang up 23andMe’s Eriksson, and asked him to run a search. In a few minutes, Eriksson was able to identify 350 people who had the mutation responsible for Gaucher’s. A few clicks more and he was able to calculate that they were five times more likely to have Parkinson’s disease, a result practically identical to the NEJM study. All told, it took about 20 minutes. “It would’ve taken years to learn that in traditional epidemiology,” Langston says. “Even though we’re in the Wright brothers early days with this stuff, to get a result so strongly and so quickly is remarkable.”
Mark Hallett, chief of the Human Motor Control section at the National Institute of Neurological Disorders and Stroke, saw Langston present his results at a recent conference and came away very impressed. “The quality of the data is probably not as good as it could be, since it’s provided by the patient,” he says. “But it’s an impressive research tool. It sounds like it’d be useful to generate new hypotheses as opposed to prove anything.”
But hypotheses are what Parkinson’s research needs more of, especially now that we can study people who, like Brin, have an LRRK2 mutation. Since some of these carriers don’t get the disease, we should try to discern why. “This is an information-rich opportunity,” Brin says. “It’s not just the genes—it could be environment or behaviors, it could be that they take aspirin. We don’t know.”
This approach—huge data sets and open questions—isn’t unknown in traditional epidemiology. Some of the greatest insights in medicine have emerged from enormous prospective projects like the Framingham Heart Study, which has followed 15,000 citizens of one Massachusetts town for more than 60 years, learning about everything from smoking risks to cholesterol to happiness. Since 1976, the Nurses Health Study has tracked more than 120,000 women, uncovering risks for cancer and heart disease. These studies were—and remain—rigorous, productive, fascinating, even lifesaving. They also take decades and demand hundreds of millions of dollars and hundreds of researchers. The 23andMe Parkinson’s community, by contrast, requires fewer resources and demands far less manpower. Yet it has the potential to yield just as much insight as a Framingham or a Nurses Health. It automates science, making it something that just … happens. To that end, later this month 23andMe will publish several new associations that arose out of their main database, which now includes 50,000 individuals, that hint at the power of this new scientific method.
“The exciting thing about this sort of research is the breadth of possibilities that it tests,” Brin says. “Ultimately many medical discoveries owe a lot to just some anecdotal thing that happened to have happened, that people happened to have noticed. It could have been the dime they saw under the streetlight. And if you light up the whole street, it might be covered in dimes. You have no idea. This is trying to light up the whole street.”
Sergey Brin is different. Few people have the resources to bend the curve of science; fewer still have spouses who run genetics companies. Given these circumstances and his data-driven mindset, Brin is likely more comfortable with genetic knowledge than most of us. And few people are going to see their own predicament as an opportunity to forge a new sort of science. So yeah, he’s different.
Ask Brin whether he’s a rare breed, and you won’t get much; on-the-record self-reflection doesn’t come easily to him. “Obviously I’m somewhat unusual in the resources that I can bring to bear,” he allows. “But all the other things that I do—the lifestyle, the self-education, many people can do that. So I’m not really that unique. I’m just early. It’s more that I’m on the leading edge of something.”
A decade ago, scientists spent $3 billion to sequence one human genome. Today, at least 20 people have had their whole genomes sequenced, and anyone with $48,000 can add their name to the list. That cost is expected to plummet still further in the next few years. (Brin is in line to have his whole genome sequenced, and 23andMe is considering offering whole-genome tests, though the company hasn’t determined a price.)
As the cost of sequencing drops and research into possible associations increases, whole genome sequencing will become a routine part of medical treatment, just as targeted genetic tests are a routine part of pregnancy today. The issue won’t be whether to look; it will be what to do with what’s found.
Today, the possibility of a rudimentary genetic test appearing on the shelves of Walgreens is headline news—delivered, inevitably, with the subtext that ordinary people will come undone upon learning about their genetic propensities. But other tests have gone from incendiary to innocuous. (Walgreens already stocks at-home paternity tests and HIV tests.) And other disclosures have gone from radical to routine. (In 1961, 90 percent of physicians said they wouldn’t tell their patients if they had cancer.) And other data points have gone from baffling to banal. (Blood pressure, LDL cholesterol, and blood sugar are now the stuff of watercooler chats.)
So, too, will it go with DNA. We’ll all find out about our propensities for disease in great detail and be compelled to work our own algorithms to address that risk. In many cases, this will be straightforward. There will be things we can do today and treatments we can undergo tomorrow.
But in some cases, undoubtedly, we may find ourselves in a circumstance like Brin’s, with an elevated risk for a disease with no cure. So we’ll exercise more, start eating differently, and do whatever else we can think of while we wait for science to catch up. In that way, Brin’s story isn’t just a billionaire’s tale. It’s everyone’s.
Mickey D’s uses varieties like the Russet Burbank, which have a nice oval shape and just the right balance of starch and sugar. Excess sugar can cause a fry to have brown spots where it’s over-caramelized, leaving a burnt taste and deviating from the uniform yellow-arches color. Just in case, the spuds are blanched after slicing, removing surplus sugar.
SODIUM ACID PYROPHOSPHATE
Taters can turn a nasty hue even after they’re fried—iron in the spud reacts with the potato’s phenolic compounds, discoloring the tissue. The phosphate ions in SAPP trap the iron ions, stalling the reaction and keeping the potatoes nice and white throughout the process.
VEGETABLE OIL
In the good old days, McDonald’s fries were cooked in beef tallow. But customer demand for less saturated fat prompted a switch to vegetable oil in the early ’90s. Here, that means oils of varying saturations combined into something reminiscent of beef tallow. There’s canola (about 8 percent saturated fat), soybean oil (16 percent), and hydrogenated soybean oil (94 percent). And to replace the essence of beef tallow? “Natural beef flavor,” which contains hydrolyzed wheat and milk proteins that could be a source of meaty-tasting amino acids.
MORE VEGETABLE OIL
That’s right, the fries get two batches of vegetable oil—one for par-frying at the factory and another for the frying bath on location. The second one adds corn oil and an additive called TBHQ, or tertbutylhydroquinone, which at high doses can cause nasty side effects in rats (mmmm … stomach tumors). McDonald’s uses this oil for all its frying, so the stuff usually sits around in big vats, which means it can go rancid as oxygen plucks hydrogens from lipids. TBHQ acts as an antioxidant, replacing those pilfered hydrogens with its own supply.
DEXTROSE
A brief dip in a corn-based sugar solution replaces just enough of the natural sweet stuff that was removed by blanching. The result is a homogeneous outer layer that caramelizes evenly. You’ll add more sugar later when you squirt on the ketchup.
SALT
Sprinkled on just after frying, the crystals are a uniform diameter—just big enough to get absorbed quickly by crackling-hot oil. Now add ketchup and you’ve achieved the hedonistic trifecta: fat, salt, and sugar.
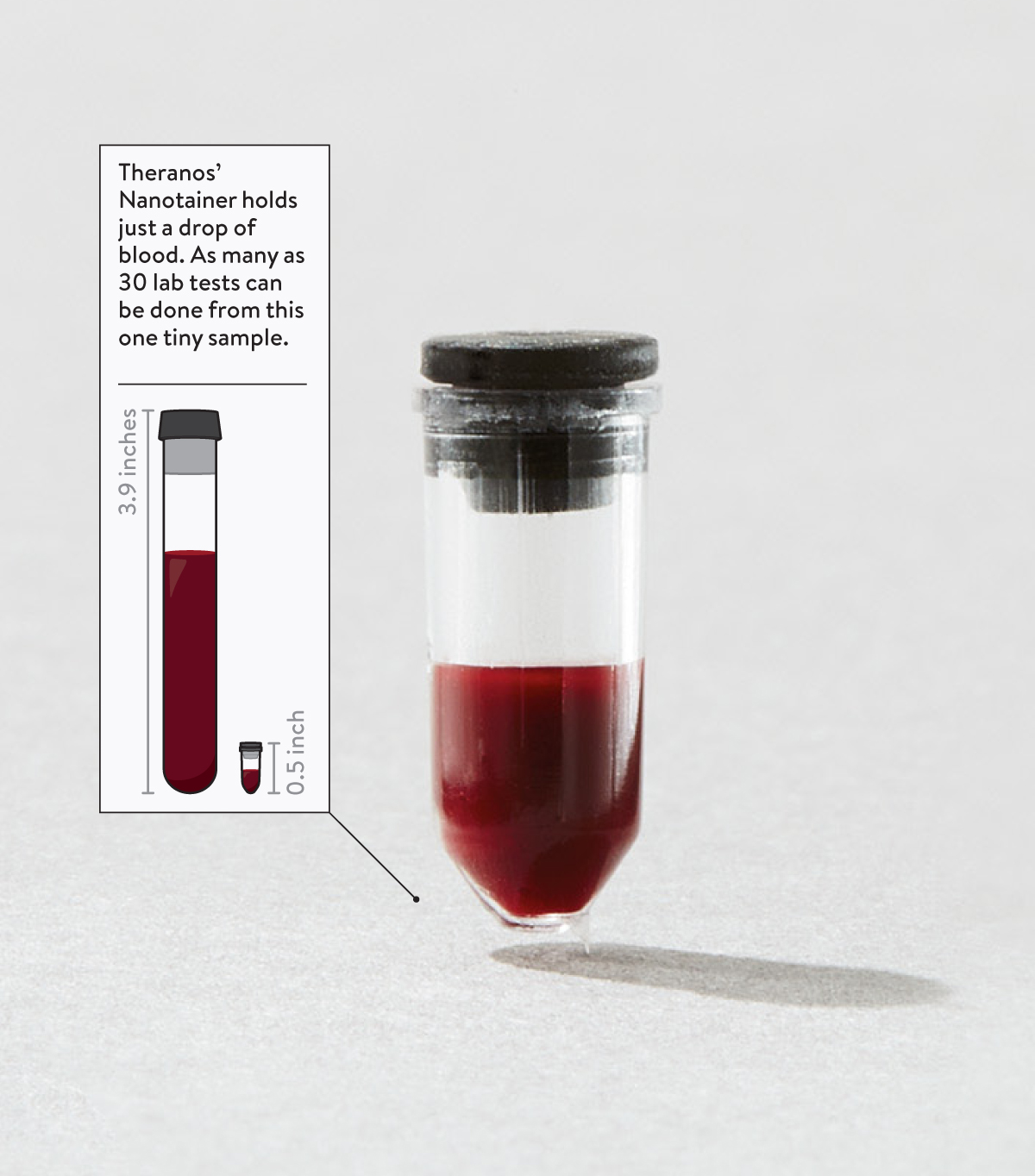
Phlebotomy. Even the word sounds archaic—and that’s nothing compared to the slow, expensive, and inefficient reality of drawing blood and having it tested. As a college sophomore, Elizabeth Holmes envisioned a way to reinvent old-fashioned phlebotomy and, in the process, usher in an era of comprehensive superfast diagnosis and preventive medicine.
That was a decade ago. Holmes, now 30, dropped out of Stanford and founded a company called Theranos with her tuition money. Last fall it finally introduced its radical blood-testing service in a Walgreens pharmacy near company headquarters in Palo Alto, California. (The plan is to roll out testing centers nationwide.) Instead of vials of blood—one for every test needed—Theranos requires only a pinprick and a drop of blood. With that they can perform hundreds of tests, from standard cholesterol checks to sophisticated genetic analyses. The results are faster, more accurate, and far cheaper than conventional methods.
The implications are mind-blowing. With inexpensive and easy access to the information running through their veins, people will have an unprecedented window on their own health. And a new generation of diagnostic tests could allow them to head off serious afflictions from cancer to diabetes to heart disease.
None of this would work if Theranos hadn’t figured out how to make testing transparent and inexpensive. The company plans to charge less than 50 percent of the standard Medicare and Medicaid reimbursement rates. And unlike the rest of the testing industry, Theranos lists its prices on its website: blood typing, $2.05; cholesterol, $2.99; iron, $4.45. If all tests in the US were performed at those kinds of prices, the company says, it could save Medicare $98 billion and Medicaid $104 billion over the next decade.
What was your goal in starting a lab-testing company?
We wanted to make actionable health information accessible to people everywhere at the time it matters most. That means two things: being able to detect conditions in time to do something about them and providing access to information that can empower people to improve their lives.
There are a billion tests done every year in the United States, but too many of them are done in the emergency room. If you were able to do some of those tests before a person gets checked into the ER, you’d start to see problems earlier; you’d have time to intervene before a patient needed to go to the hospital. If you remove the biggest barriers to these tests, you’ll see them used in smarter ways.
What was your motivation to launch Theranos at the age of 19? What set you on this road?
I definitely am afraid of needles. It’s the only thing that actually scares me. But I started this company because I wanted to spend my life changing our health care system. When someone you love gets really sick, most of the time when you find out, it’s too late to be able to do something about it. It’s heartbreaking.
You’re not alone in your fear of needles.
Phlebotomy is such a huge inhibitor to people getting tested. Some studies say that a substantive percentage of patients who get a lab requisition don’t follow through, because they’re scared of needles or they’re afraid of worrying, waiting to hear that something is wrong. We wanted to make this service convenient, to bring it to places close to people’s homes, and to offer rapid results.
Why the focus on rapid results?
We can get results, on average, in less than four hours. And this can be very helpful for doctors and patients, because it means that someone could, for example, go to a Walgreens in the morning to get a routine test for something their doctor is tracking, and the physician can have the results that afternoon when they see the patient. And we’re able to do all the testing using just a single microsample, rather than having to draw a dedicated tube for each type of test.
So if I got a blood test and my doctor saw the results and wanted other tests done, I wouldn’t have to have more blood drawn?
Exactly. And on their lab form, the physician can write, “If a given result is out of range, run this follow-up test.” And it can all be done immediately, using that same sample.
Some conventional tests, like pH assays, can be done quickly. Others, like those that require culturing bacteria or viruses, can take days or even weeks. Are there some tests that take Theranos longer? Can everything really be turned around in four hours?
Yes, we had to develop assays or test methodologies that would make it possible to accelerate results. So we do not do things like cultures. In the case of a virus or bacteria, traditionally tested using a culture, we measure the DNA of the pathogen instead so we can report results much faster.
Where do you see this making a big difference?
Fertility testing is a good example. Most people pay for it out of pocket, and it can cost as much as $2,000. These tests provide the data you need to figure out someone’s fertility, and some women can’t afford them. Our new fertility panel is going to cost $35. That means women will be able to afford the tests. They’ll be able to better manage the process and take some of the stress out of trying to conceive.
What are you doing to ensure the accuracy of your testing?
The key is minimizing the variability that traditionally contributes to error in the lab process. Ninety-three percent of error is associated with what’s called pre-analytic processing — generally the part of the process where humans do things.
Such as?
Manually centrifuging a sample or how much time elapses before you test the sample, which brings its decay rate into play.
So how do you avoid these potential errors?
There’s no manual handling of the sample, no one is trying to pipette into a Nanotainer, no one is manually processing it. The blood is collected and put into a box that keeps it cold. The very next thing that happens is lab processing, and that’s done with automated devices at our centralized facility with no manual intervention or operation.
How can improved processes actually save lives?
We’ve created a tool for physicians to look at lab-test data over time and see trends. We don’t usually think about lab data this way today. It’s “Are you in range, or are you out of range?” Instead, we like to think, “Where are you going?” If you showed me a single frame from a movie and asked me to tell you the story, I wouldn’t be able to do it. But with many frames, you can start to see the movie unfold.
How else can you use this technology?
Many, many years of work went into making this possible. We started our business working with pharmaceutical companies. Because we made it possible to get data much faster, they could use our infrastructure to run clinical trials. They were also able to run what’s called an adaptive clinical trial, where based on the data, they could change the dosing for a patient in real time or in a premeditated way, as opposed to waiting a long period and then deciding to change a dose.
In the long run, what impact will your technology have?
The dream is to be able to help contribute to the research that’s going on to identify cancer signatures as they change over time, to help intervene early enough to do something about an illness.
Will people become more used to gathering and examining their own health data?
No one thinks of the lab-testing experience as positive. It should be! One way to create that is to help people engage with the data once their physicians release it. You can’t do that if you don’t really understand why you’re getting certain tests done and when you don’t know what the results mean when you get them back.
It drives me crazy when people talk about the scale as an indicator of health, because your weight doesn’t tell you what’s going on at a biochemical level. What’s really exciting is when you can begin to see changes in your lifestyle appear in your blood data. With some diseases, like type 2 diabetes, if people get alerted early they can take steps to avert getting sick. By testing, you can start to understand your body, understand yourself, change your diet, change your lifestyle, and begin to change your life.
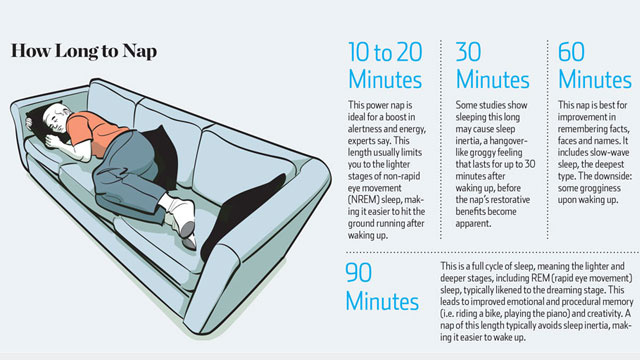
„Taking a nap, we’ve seen time and again, is like rebooting your brain. Everyone likes to get a quick nap in every now and then, but napping may be as much of an art as it is a science. The Wall Street Journal offers recommendations for planning your perfect nap, including how long to nap and when.
The sleep experts in the article say a 10-to-20-minute power nap gives you the best “bang for your buck,” but depending on what you want the nap to do for you, other durations might be ideal. For a quick boost of alertness, experts say a 10-to-20-minute power nap is adequate for getting back to work in a pinch.
For cognitive memory processing, however, a 60-minute nap may do more good, Dr. Mednick said. Including slow-wave sleep helps with remembering facts, places and faces. The downside: some grogginess upon waking.
“If you take it longer than 30 minutes, you end up in deep sleep. Have you ever taken a nap and felt worse when you woke up? That’s what’s happening — you’re sleeping too long and you’re going into a stage of sleep that’s very difficult to get out of.” – Dr. Michael Breus
Finally, the 90-minute nap will likely involve a full cycle of sleep, which aids creativity and emotional and procedural memory, such as learning how to ride a bike. Waking up after REM sleep usually means a minimal amount of sleep inertia, Dr. Mednick said.
In fact, a study published in PubMed in 2002 found that napping even for 5-10 minutes creates a heightened sense of alertness and increased cognitive ability in comparison to no nap. So really, you want to be taking a 10-20 minute nap for a quick recharge, or a 60-90 minute nap for a deep sleep rejuvenation.
In addition to those recommendations, one surprising suggestion is to sit slightly upright during your nap, because it will help you avoid a deep sleep. And if you find yourself dreaming during your power naps, it may be a sign you’re sleep deprived.“

 DeepMind cofounder Mustafa Suleyman.DeepMind
DeepMind cofounder Mustafa Suleyman.DeepMind A technician examines an OCT scan.DeepMind
A technician examines an OCT scan.DeepMind DeepMind’s AI analysing an OCT scan.DeepMind
DeepMind’s AI analysing an OCT scan.DeepMind A patient having an OCT scan.DeepMind
A patient having an OCT scan.DeepMind